What I Wish I Knew About Internal Medicine Training

Outline
- The Gap Between IMT on Paper and IMT in Real Life
- Get Your Exam Strategy Right Early
- PACES: Timing Matters More Than People Think
- Do Not Just Get Signed Off. Become Competent
- You May Need to Chase Procedures, Clinics, and Opportunities
- Build Your Portfolio Early
- Choose Audit and QI Work That Solves Real Problems
- Think Early About Your Higher Specialty Direction
- The Step Up From IMT2 to IMT3
- What I Wish I Had Known at the Start
The Gap Between IMT on Paper and IMT in Real Life
If you look at the IMT curriculum, it reads like a well-organised training programme. You rotate through specialties, you gather competencies, you sit exams, you build a portfolio, and you come out the other end as a medical registrar. On paper, it makes sense.
In practice, it did not always feel like that.
A lot of my time in IMT1 and IMT2 was spent on service provision. Ward rounds, clerking, discharge summaries, chasing scans, dealing with the admin that keeps a hospital running. I am not saying that work is without value, because it is how you learn the rhythm of acute medicine and how to manage a caseload. But it is easy for weeks to go by where you have not done a single procedure, not attended a clinic you wanted to, and not had a meaningful teaching interaction, because the job simply swallowed up the day.
I was on a rotation through a senior-led tertiary centre for most of IMT1 and IMT2, and I’ll be honest: for a lot of that time, I felt like I had no real impact on patient outcomes. Decisions were made above me, plans were already in motion before I arrived on the ward, and my contribution often felt like execution rather than thinking. That changed significantly in IMT3, and I will get to that later in the piece, but the point I want to make here is that the training value of IMT is not automatic. It does not arrive just because you are on the rotation.
What I came to realise is that the trainees who got the most out of IMT, including myself once I worked it out, were usually the ones who were deliberate about it. That meant actively chasing procedures, booking into clinics, making use of sim sessions, and treating each posting as a limited window to learn specific things rather than just turning up and doing the job. None of that is written into the rota for you. If you wait for the programme to hand you the training, you will probably end up with gaps you did not expect.
I do not say this to be critical of IMT as a programme. There are good rotations, good departments, and good supervisors. But the structure alone does not guarantee that you will come out feeling competent and confident. That part is largely on you, and knowing that early makes a real difference.
Get Your Exam Strategy Right Early
MRCP is one of the defining challenges of IMT, and the earlier you take it seriously, the better. This is not one of those exams you can wing with a couple of weeks of cramming. It is genuinely difficult, and fitting revision around the rhythm of the job, with nights, post-call recovery days, and unpredictable rotas, is harder than most people expect going in.
I completed Part 1 and Part 2 before starting IMT, which meant I entered training with the written exams behind me. Not everyone will be in that position, and the timing advice I give here comes from reflecting on my own experience and talking to colleagues about what worked for them.
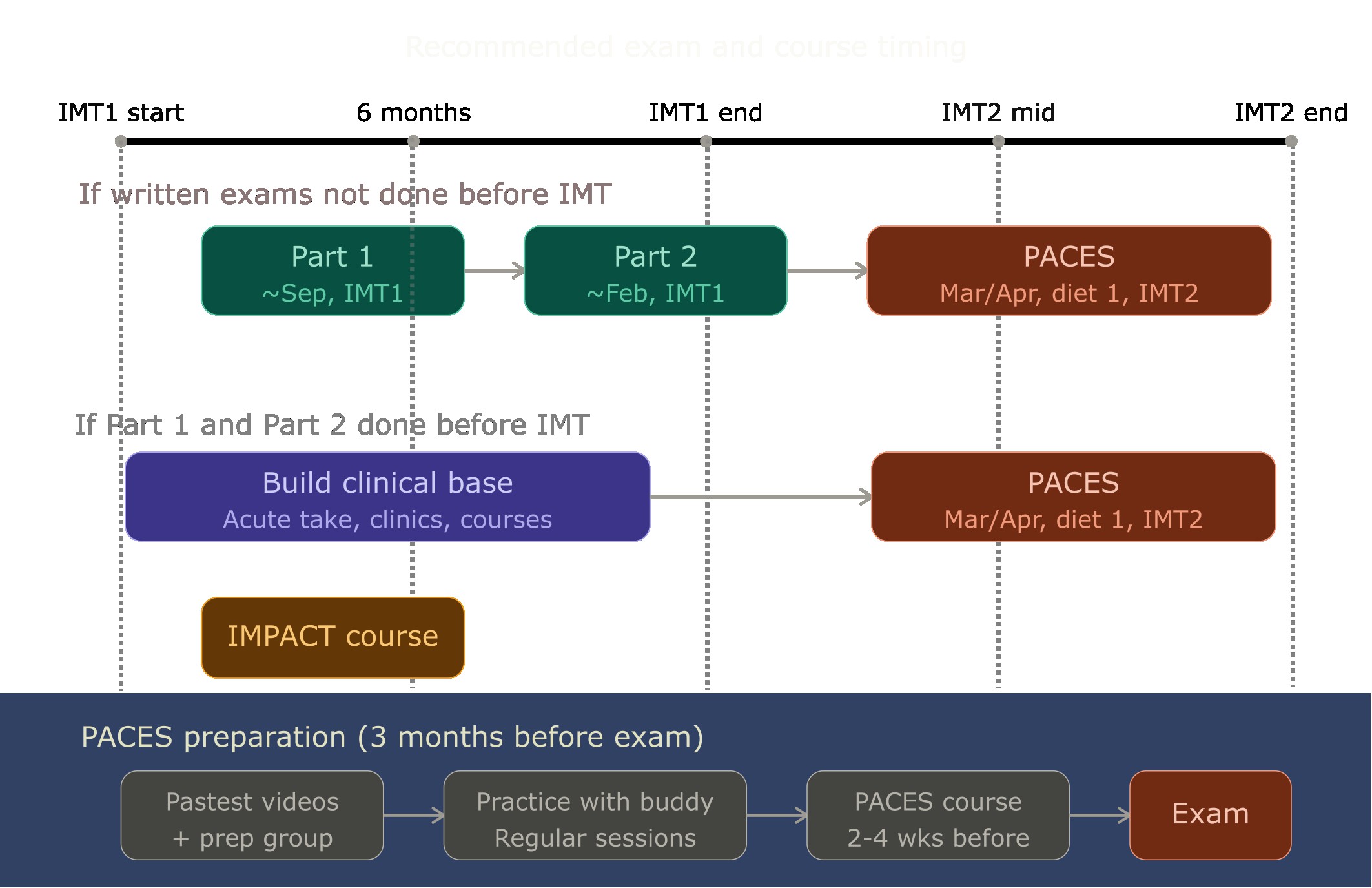
If you have not sat Part 1 before starting IMT, I would suggest doing it early. A realistic target is Part 1 around September, about two months into IMT1, and Part 2 around February of the next year. Part 1 and Part 2 are structured the same way, so whatever approach works for you on one will broadly work for the other. The goal is to get both done before the end of IMT1, so you are not carrying written exams into IMT2 alongside PACES preparation.
If you have already passed both written exams before IMT, you are in a good position, but I would encourage you not to rush straight into PACES. I made that mistake, and I cover it properly in the next section.
Regardless of your timing, here is the study approach that worked for me. I appreciate it might not suit everyone, but this is the system I stuck with.
I used Passmedicine as my primary question bank. The biggest mistake I saw people make was trying to cover multiple question banks at the same time, jumping between Passmedicine, Pastest, and others without properly completing any of them. I found it more effective to commit to one bank first, work through it completely, and then go back over the questions I got wrong. After that, I subscribed to Pastest and used their mock exams specifically to calibrate my level and check whether I had actually understood the concepts rather than just memorised the answers. I also did the sample questions from the MRCP website. In the last two weeks before the exam, I was doing nothing but mocks.
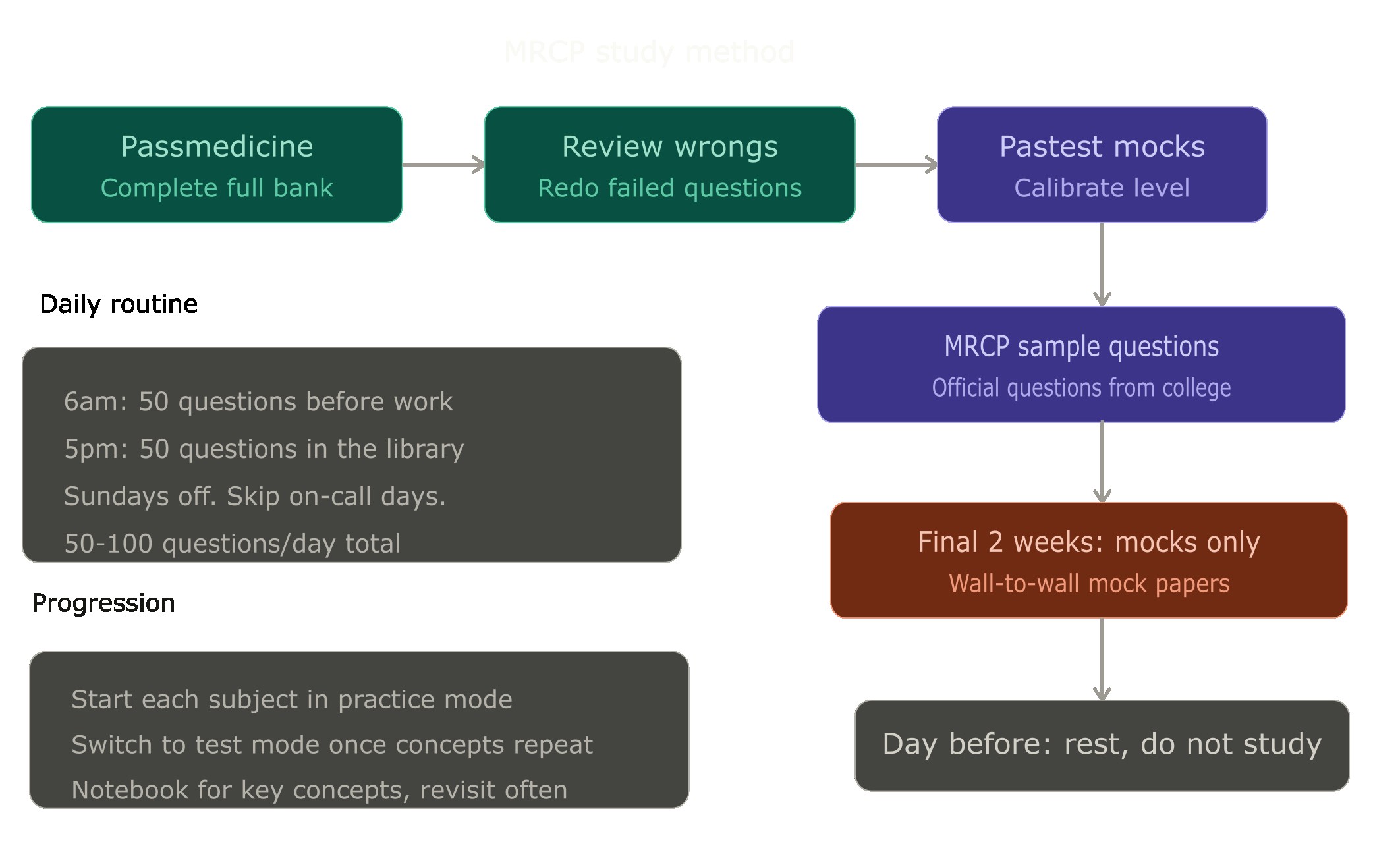
My daily routine during the preparation period was roughly 50 to 100 questions per day, except when I was on calls. I had Sundays off completely. I would wake up at 6am and do about 50 questions before work, then after finishing at 5pm I would go to the library and do another 50. When I started a new subject in Passmedicine, say cardiology, I was much slower initially. It might take me 40 minutes to get through 20 questions in the first few hundred. But as the concepts started repeating and I got more familiar with the patterns, I could do 40 questions in the same time. I mention this because it is easy to feel disheartened early on when you are moving slowly, but that is normal and it gets better.
I worked through each subject in practice mode first, where I could see the answer and explanation after every question. Any concept I did not understand, I would watch a YouTube video to get a clearer picture. Nowadays you could also use AI tools like ChatGPT to explain things more clearly, and I think that is a reasonable addition. I kept a notebook where I wrote down concepts I needed to remember and revisited it regularly. Once I had a good grasp of most of the material in a subject and things were becoming repetitive, I switched to test mode: 40 questions at a time, answers at the end.
If you can, try to arrange study leave for your final week of preparation. That last stretch is when you want to be locked in, doing as many mock papers as possible. And on the day before the exam itself, I would suggest not studying at all. By that point, you know what you know. Anything extra is unlikely to change the outcome and may just add stress.
If you are not successful on your first attempt, the main thing I would say is do not treat the reattempt casually. Look at your score sheet, identify the sections where you underperformed, and speak to a senior colleague about it. If you used Passmedicine the first time, it is probably reasonable to switch to Pastest for the reattempt and go through the whole bank properly. But regardless of what you use, approach the resit as if you are doing it for the first time. The two weeks before the exam should be wall-to-wall mocks, just like the first attempt.
Most people need somewhere between six weeks and three months of serious preparation. That is evenings and weekends, consistently. It is not a small ask alongside a full clinical job, and I think it helps to know that upfront so you can plan your time rather than just hoping it works out.
If your baseline is not strong and you are struggling with question banks even after getting through half of them, it might be worth considering a course or joining a study group to help with the concepts. But more often than not, in my experience, working through the questions methodically without jumping between banks was enough.
PACES: Timing Matters More Than People Think
PACES is a different beast from the written exams, and I think it deserves its own section because the way you prepare for it, the timing of when you sit it, and the mindset you bring to it all matter more than people tend to realise.
I want to start with my own experience here, because the timing lesson is one I learned the hard way.
I had Part 1 and Part 2 done before starting IMT, so I went into PACES quite early in IMT1. At the time, it felt like the logical next step: the written exams were out of the way, so why not press on? Looking back, that was a mistake. I did not have enough acute medical experience at that point for things to feel natural at the bedside. The clinical pattern recognition, the confidence with examination routines, the instinct for how to present and communicate findings clearly: a lot of that comes from sustained exposure to the acute take and to real patients over time, and I simply had not had enough of it yet.
I failed PACES twice before passing on my third attempt. Both times, I failed by a single mark. I was scoring above 85% overall in the exam, passing the majority of stations comfortably, but failing by one mark in a specific domain that was needed to pass. The exam is structured so that a mistake in a key domain can fail you even if your total score is well above the pass mark. That is just how it works, and it can feel brutal.
Part of what went wrong was readiness. But part of it was also mindset. In my first two attempts, I went in thinking I just needed to pass most of the stations. That sounds reasonable, but it was actually detrimental. The structure of the exam means you cannot afford to be average in any domain. After my second failure, I recalibrated. I started preparing with the goal of scoring 100% in every station, not because I expected perfection, but because that was the surest way to reduce the risk of losing a single mark in a critical domain. That mindset shift, combined with the extra clinical maturity I had built up by that point, made a genuine difference. I wish I had adopted both earlier.
Based on my experience and from talking to colleagues, the timing I would now recommend is this: aim for PACES around late March or April in diet 1 of the year, roughly seven to eight months into IMT2. If you need to retake, diet 2 runs from May to August in the same year, which gives you a second opportunity without losing too much time. If you have already passed Part 1 and Part 2 before starting IMT, I would strongly suggest not rushing into PACES in IMT1 the way I did. Use that time instead. Do the IMPACT course. Get as much acute take exposure as you can. Attend clinics, build procedural confidence, and let your clinical skills mature. A lot of what helps in PACES develops naturally from that kind of sustained clinical work, and by the time you have had a good stretch of it, more than you might expect will come to you instinctively. IMT2 gives you that foundation.
Three months is a realistic preparation window for most people. I would suggest starting with the Pastest videos to get a feel for the format and standard expected, then joining a PACES preparation group and actually engaging with it rather than just being on the WhatsApp. Having a PACES buddy to practise with regularly goes a long way. I found it genuinely useful to rehearse stations with someone who could give honest feedback, rather than just reading about examination technique in isolation. Going on a PACES course about two to four weeks before the exam also helped me get into the right mindset and sharpen things up.
One practical tip: after booking, you can email the PACES college to request a specific date range for your exam. If you have a reasonable justification, they are often willing to accommodate it. It is worth doing, because the timing of your exam relative to your preparation and your rota can make a real difference.
If you do have to resit, ask for your marksheet and go through it with a senior colleague. Identify the areas where you dropped marks, put real effort into those specific domains, and then prepare as though you are sitting it for the first time. Do not go in thinking you only need to fix one or two things. Go in fresh.
I eventually got through PACES just before IMT3, and by that point I felt genuinely ready. But I honestly got quite engrossed with the exam during IMT2 and did not do much else during that period. If I had it to do again, I would use late IMT1 and early IMT2 to get as much learning and course attendance in as possible before PACES preparation took over. Once you are deep in revision, it is hard to make time for anything else.
Do Not Just Get Signed Off. Become Competent
This is something that only became really clear to me in IMT3, and I think it is one of the most important points in this piece.
There is a difference between having a procedure signed off in your portfolio and actually being confident enough to do it independently when it matters. The portfolio says you can do it. But the portfolio does not know whether you have done it once in a controlled setting or twenty times under real conditions. And when you are the medical registrar on the acute take and someone needs a procedure at 2am, it is the second kind of competence that counts.
The clearest example I can give is lumbar puncture. I got signed off for LPs in IMT1 through a simulation session and a supervised real case. On paper, I was competent. But because I did not do enough of them afterwards during IMT2, the skill was not truly embedded. By the time I started IMT3, I had to admit to myself that I was less confident with it than my portfolio suggested.
What helped was not another sign-off, but deliberate repetition. In a later posting, I made a point of getting supervised exposure with clinicians who performed lumbar punctures frequently. That repeated practice exposed a technical flaw in my approach and corrected it. More importantly, it rebuilt the kind of confidence that only comes from doing a procedure enough times under supervision.
That is the lesson I would emphasise. If a procedure matters to your future role, do not stop at being signed off. Chase the opportunities, ask for supervision, and keep going until the skill feels reliable under pressure.
The same principle applies to other procedures. Arterial lines, central lines, ascitic drains, pleural drains. All of these require mastery of the Seldinger technique, and there is no substitute for repetition. During my ITU block, I stayed back on several occasions specifically to get the numbers in for arterial and central lines. I do not regret a single one of those late finishes. Each one made me a little more confident, and that confidence mattered when I was eventually running the take on my own.
The broader point is this: try to do enough of each procedure that you are genuinely confident performing it whenever you need to, not just enough to get the form signed. That is not always easy given rota pressures and the way some services are structured, but the difference it makes to how you feel as a medical registrar is significant.
You May Need to Chase Procedures, Clinics, and Opportunities
One of the things nobody really tells you at the start of IMT is that most training opportunities will not come to you. You have to go looking for them. This is not a vague “be proactive” point. I want to explain what that actually looked like in practice, because I think the detail matters.
For procedures, I started early and made a deliberate effort to use every posting for the opportunities it was best placed to offer. A lot of hospitals organise simulation sessions where you can practise procedures on mannequins before doing them on patients, and I made sure to attend those whenever they were available. What helped was also getting familiar with the specific instruments used in the trust, because kit varies between hospitals and it is easier to focus on the patient when you are not also figuring out the equipment.
Some procedures are harder to get exposure to because specialist non-doctor teams run the service. DCCV is a common example. If that is the case in your trust, you need to actively get into those clinics and ask to be involved. It will not happen by default.
As I mentioned earlier, my ITU block was where most of my procedural volume came from, and I would strongly recommend treating your ITU rotation as a concentrated window for building that confidence. The opportunities there are not spread thinly the way they tend to be on general medical wards.
I also wish someone had told me about the IMPACT course earlier. It is a two-day course that combines multiple simulation scenarios and covers A-to-E assessment, diagnosis of acutely unwell medical patients, and important diagnostic procedures done in IMT. I ended up completing it later than I should have. Ideally, finishing it in F2 or early IMT1 would be best. If your trust already has strong sim and skills sessions, some of the content will be repetitive, but repetition and mastery go hand in hand, and the course brings it together in a structured way that is hard to replicate piecemeal.
For clinics, the approach that worked for me was being deliberate about access. Before a new posting started, I would find out which days the relevant clinics ran and who the supervising consultant was. Then I would contact the consultant ahead of time to let them know I would be attending, so they were expecting me and could plan to involve me in seeing patients rather than just having me sit in. That small step, just a message or an email in advance, made a noticeable difference to how useful the clinic time actually was. When you just turn up unannounced, it is easy to end up observing rather than doing. When the consultant knows you are coming and what you want to get out of it, they are far more likely to give you cases and let you lead.
I also found it helpful to keep track of which clinics I still needed and to plan my requests around what each posting could realistically offer. Not every rotation has the same clinic access, so treating each one as a specific window for specific exposures helped me avoid getting to the end of a block and realising I had missed an opportunity that was right there.
None of this is complicated, but it does require effort and a bit of organisation. The training programme gives you the placements. What you do within those placements, who you contact, what you ask for, whether you follow up, is largely up to you. In my experience, the difference between trainees who came out of IMT feeling well-prepared and those who felt they had gaps was often not ability or intelligence, but how actively they had pursued the opportunities that were technically available to everyone.
Build Your Portfolio Early
Portfolio evidence does not gather itself, and the longer you leave it, the more stressful it becomes. I have seen colleagues scrambling in the final months of a training year to get assessments completed that could have been done months earlier with a quick conversation. The work itself is not difficult. What catches people out is not doing it as they go.
The practical reality is this: after a clinic session or a shift on the acute take, speak to the registrar or consultant you worked with and ask if you can send them a ticket to sign off, confirming your competency and giving feedback. It takes them a few minutes to complete, and it saves you from trying to chase the same person weeks later when neither of you can remember the detail. Get into the habit of doing this early and doing it consistently. MSF forms, OPCATs, mini-CEX assessments: request them as you go rather than batching them up at the end.
ACATs on the acute take deserve a specific mention because they can be difficult to arrange in the traditional way. The classical format, where a senior directly observes your clerking and management of a few cases, is hard to set up when the take is busy and everyone is moving quickly. What I found worked better was a practical alternative: I would keep a list of patients I had clerked during the acute take, then afterwards find the consultant who had post-taked them. I would ask if we could discuss the cases, review my management plan, and get their feedback both in person and via the acute take assessment form. It is not the textbook ACAT setup, but it captures real clinical work and genuine feedback, which is what the assessment is supposed to reflect. Some deaneries also have dedicated ACAT clinics where you can book into a session with a consultant specifically to discuss cases you have seen on the take, get feedback, and get an ACAT completed. If that exists in your deanery, make use of it.
While I am on the topic of protecting your training time, a few things on leave that I think are worth knowing. Book your annual leave well ahead. Make sure you are actually using your study leave entitlement, because it is easy to let it slip when you are busy. And one thing that caught me by surprise initially: if you book study leave that falls on a zero day or on a day that would have been annual leave, you are entitled to claim that day back in lieu. Try not to give away your rest days for study. You should be well protected as a trainee, and knowing the rules helps you make sure that actually happens.
Choose Audit and QI Work That Solves Real Problems
Audit and QI are part of the training requirements, and most people know they need to do them. The difference, in my experience, is between projects that are done purely to tick a box and projects that are based on real problems you have noticed in your day-to-day work. The second kind is more useful, more interesting, and usually better received.
My approach whenever I started a new posting was to pay attention to the bottlenecks and annoyances in the system. What was slowing things down? What were people complaining about? What seemed wasteful or unnecessarily complicated? If I needed something quickly, I would ask the registrars what projects they were already working on and whether I could contribute. But the best audits I did came from things I noticed myself.
The clearest example was during my oncology block. I noticed that a lot of blood tests were being ordered automatically for stable inpatients on the ward, even when there was no clear clinical indication for them. I went to work exploring what was driving this: standing orders, habit, lack of review. I put together an intervention to reduce unnecessary blood testing, and it was well received by the department. The trust-wide saving potential was significant. It was not a complicated project, but it addressed a real problem, and that made it easier to write up, easier to present, and more credible when I talked about it.
The practical steps for getting audit and QI work off the ground are fairly straightforward. Identify a registrar and consultant who are willing to supervise, write a brief proposal, and contact the QI or governance team in the department to register the project. Once you have results, present them at the local QI meeting. If the work is strong enough, try submitting to a regional QI meeting as well. You can even publish in the BMJ Open Quality, which adds a publication to your name alongside the audit itself.
One thing I noticed is that there are problems worth solving in almost every department you join. You just have to be a bit attentive to find them. If you keep your eyes open during the first week or two of a new posting and ask the right questions, the project ideas tend to present themselves.
Think Early About Your Higher Specialty Direction
This is a point I think is worth raising, even though I know not everyone will agree, and I recognise it is easier to say in hindsight.
One thing I noticed during IMT was that a few of my colleagues did not know what higher specialty they wanted to pursue, even well into IMT2. On reflection, I think part of the reason is structural. In surgical training, CST programmes are often themed from the start. A person beginning CT1 surgery will generally know which subspecialty they are aiming for, and their rotations are shaped around that. In medicine, that does not really exist. You rotate through a range of specialties, and while that breadth is valuable, it also means there is no built-in pressure to decide early. A lot of people end up postponing the decision, and that can make it harder to optimise your portfolio, your projects, and your clinical exposure in time for applications.
For me, even before starting IMT, I already knew I was not going to do paediatrics or obstetrics and gynaecology. The only surgical specialty I seriously considered was cardiothoracic surgery, but one look at the competition ratio in the UK was enough to put me off. Cardiology gave me a close flavour of what I liked about cardiothoracic, and that made the decision relatively straightforward.
I also told myself something that helped: subspecialties are like every other job, and each one will have its annoying bits. Once I accepted that, it became much easier to commit rather than endlessly weighing up options. I am not sure that reasoning will work for everyone, but it worked for me.
The application timeline is worth knowing early. For group 2 specialties, applications open in November, roughly three months into IMT2. For group 1 specialties, it is November, three months into IMT3. If you know your direction even loosely, you can start shaping your portfolio, audits, and clinical exposure toward it well in advance. If you do not know yet, that is fine, but I would encourage you to at least start narrowing things down rather than keeping everything open indefinitely.
One other thing I would add: I think it is important to have interests beyond your clinical specialty. It gets boring doing anything repeatedly, and having other projects, whether that is research, quality improvement, teaching, digital health, or something else entirely, makes it possible to build a varied job plan on CCT. The consultants I have seen who seem most fulfilled are not the ones doing a single routine five days a week. They are the ones with different things to engage with across the week.
The Step Up From IMT2 to IMT3
I got promoted to medical registrar after a successful ARCP outcome in IMT2, and I expected it to be really difficult. To be clear, I did have acute take exposure in IMT1 and IMT2, and I was well supported. But in a senior-led tertiary centre, the decision-making often sat above me, and for a lot of that time I felt like I was not making much difference to patient outcomes. One thing I tried to do when I could was speak with the med reg on shift and run my unclear plans past them, which helped me learn even when I was not the one driving the decisions. But the overall feeling was still that my contribution was more about execution than independent thinking. So the idea of suddenly being the person everyone called for advice felt daunting.
Interestingly, it was not as bad as I imagined.
What surprised me was how much I actually knew. When you are covering as the medical registrar and people from across the local region are calling to ask for advice on managing their patients, you realise that the knowledge base you have built up over two years of acute take exposure, exam preparation, and clinical work is more substantial than you thought. That was a genuinely reassuring discovery, and I think a lot of new medical registrars have a similar experience once they get past the initial anxiety.
That said, there were things that helped me settle in. One was how I introduced myself. When I was newly working as a medical registrar and calling consultants for advice out of hours, I would introduce myself as an IMT3. It was a small thing, but it helped them understand my level, and consultants were generally very reasonable about giving support and guidance when they knew where I was in training. Do not feel like you have to pretend you have been doing this for years. There is usually support available for new medical registrars, and it is worth using it.
The single most useful thing I did during IMT3 for my own development was keeping a private list of patients I reviewed, saw, or gave advice on during my shifts. After each set of shifts, I would go back and look at the outcomes: what happened to the patient, whether my recommendations turned out to be right, what the eventual diagnosis or management plan was. This was incredibly helpful in making me grow quickly. I could see the effect of my decisions in real patients and learn from both the good calls and the ones I would do differently. I would strongly recommend this to anyone starting as a medical registrar.
On practical tools, I found that hospital guidelines were the first place to look for almost everything. As a medical registrar running the take, you will encounter a lot of things that are not pneumonia and UTI, and you will need to look up management for conditions you have not seen regularly. Having quick access to your trust’s guidelines makes a real difference. For cases that are not covered locally, UpToDate is comprehensive and evidence-based, and I used it frequently for troubleshooting. BMJ Best Practice is a reasonable alternative. MDCalc is useful for quick clinical calculations. BNF is essential for drug doses and interactions. I also found the Renal Handbook particularly helpful for managing end-stage CKD patients. These are not glamorous recommendations, but having these resources accessible on your phone or work computer makes the take run more smoothly.
IMT3 was significantly better than the earlier years for me. As I described at the start of this piece, IMT1 and IMT2 often felt like I was contributing without really driving decisions. In IMT3, with the responsibility of managing the acute take, that changed. I saw myself grow rapidly. I felt more confident, I felt more useful, and I genuinely enjoyed the work. I really do enjoy working on the acute take. If you are in IMT1 or IMT2 right now and wondering whether it gets better, in my experience it does, and by a meaningful margin.
What I Wish I Had Known at the Start
If I could go back and tell myself a few things at the beginning of IMT, these are the ones that would have made the most difference.
First, the gap between having something signed off and actually being competent at it is real, and it matters. Portfolio completion and clinical confidence are not the same thing. I learned this most clearly with lumbar punctures, but the principle applies to almost everything. Do not confuse a tick in a box with readiness.
Second, nobody hands you the training. The programme gives you placements, but what you extract from them is largely down to you. The trainees I saw get the most out of IMT were the ones who chased procedures, contacted consultants ahead of clinics, kept track of what they still needed, and treated each posting as a window for specific things. That deliberateness made a real difference.
Third, do not rush through the exams just because you can. I sat PACES too early, and it cost me two attempts that I could have avoided with more clinical maturity. Getting Part 1 and Part 2 done quickly is sensible. Getting into PACES before you are ready is not.
Fourth, use AI in your training. I do not mean this in a vague futuristic sense. I mean practically, right now. Use it to improve the grammar in your portfolio reflections. Use it to brainstorm audit and research project ideas. If your trust allows it, use it as an ambient scribe for your clinics. OpenEvidence is a particularly good evidence-backed AI tool that I use in my clinical workflow, and I would recommend it.
Fifth, IMT3 is where it comes together. If you are in the earlier years and feeling like the work is repetitive or that you are not growing, hold on. The step up to medical registrar brings a level of responsibility and decision-making that accelerates your development in a way the first two years do not. I went from feeling like I had no impact to genuinely enjoying the acute take and feeling confident in my clinical judgement. That shift was real.
IMT is often talked about as something to endure, and I understand why. The exams are hard, the rotas are demanding, and the portfolio can feel like admin for the sake of admin. But the outcome is not as bleak as it is generally painted. On completion, you can work as a medical registrar in any hospital, and the skill set you build is transferable well beyond clinical medicine. It is a stepping stone to the medical specialty you want, and if you are deliberate about how you use it, it can be a genuinely formative period.
I wish you the best in your IMT journey.