First Impressions: Life as a Cardiology Registrar
In this post
- The oncalls
- The day job
- Learning curve in the cath lab
- Echo: a work in progress
- Beyond the procedures
- Two months in
The oncalls
I started cardiology training as an ST4 on 25 March 2026, moving from an IMT3 post at a tertiary centre to a district general hospital. The two are quite different environments, and not just in the ways I expected.
The oncalls have been tough. For my first set of nights, I was the only medical registrar covering the ED, SDEC and the wards simultaneously. In all my time on the Mersey rotation, I had not come across a rota structured quite like this. The shifts end with a particular kind of exhaustion, the sort that comes not just from the clinical load but from knowing there is no one to split it with.
This post is not really about that. But it would be dishonest to write about starting cardiology training without acknowledging it, because the two things exist in the same week, often the same 24 hours.
The day job
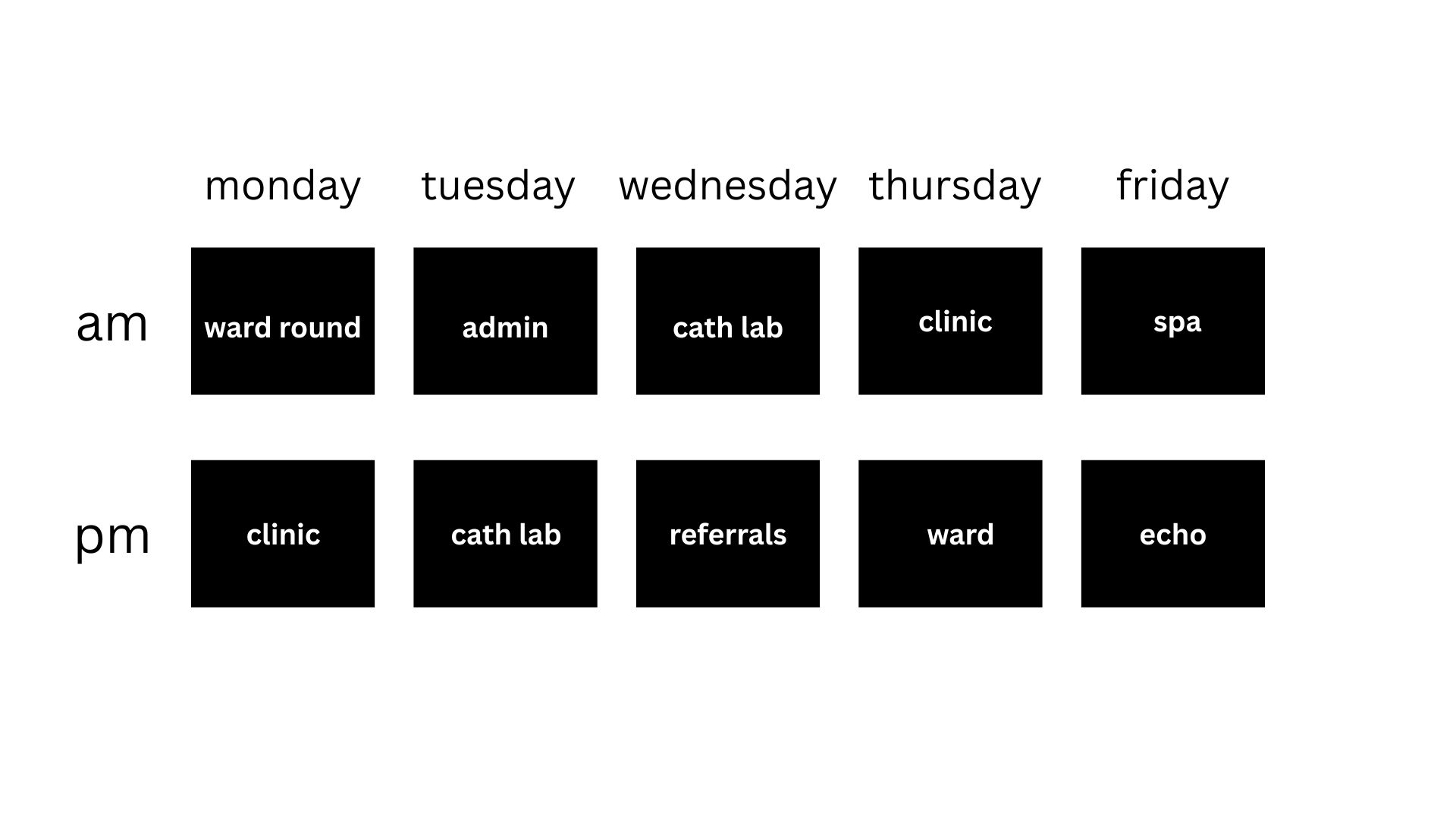
Outside of the oncalls, the day job feels genuinely different from IMT. The job plan is properly structured around training: Monday ward rounds and clinic, Tuesday admin and scan reporting, Wednesday in the cath lab, Thursday rapid access chest pain clinic and ward support, Friday self-development and echo. It reads like a training programme, because it actually is one.
That was not always my experience in IMT, where the rota could feel more like service provision with training grafted on. Here, the week has a shape, and most days I finish knowing I have learned or done something specific to cardiology.
Learning curve in the cath lab
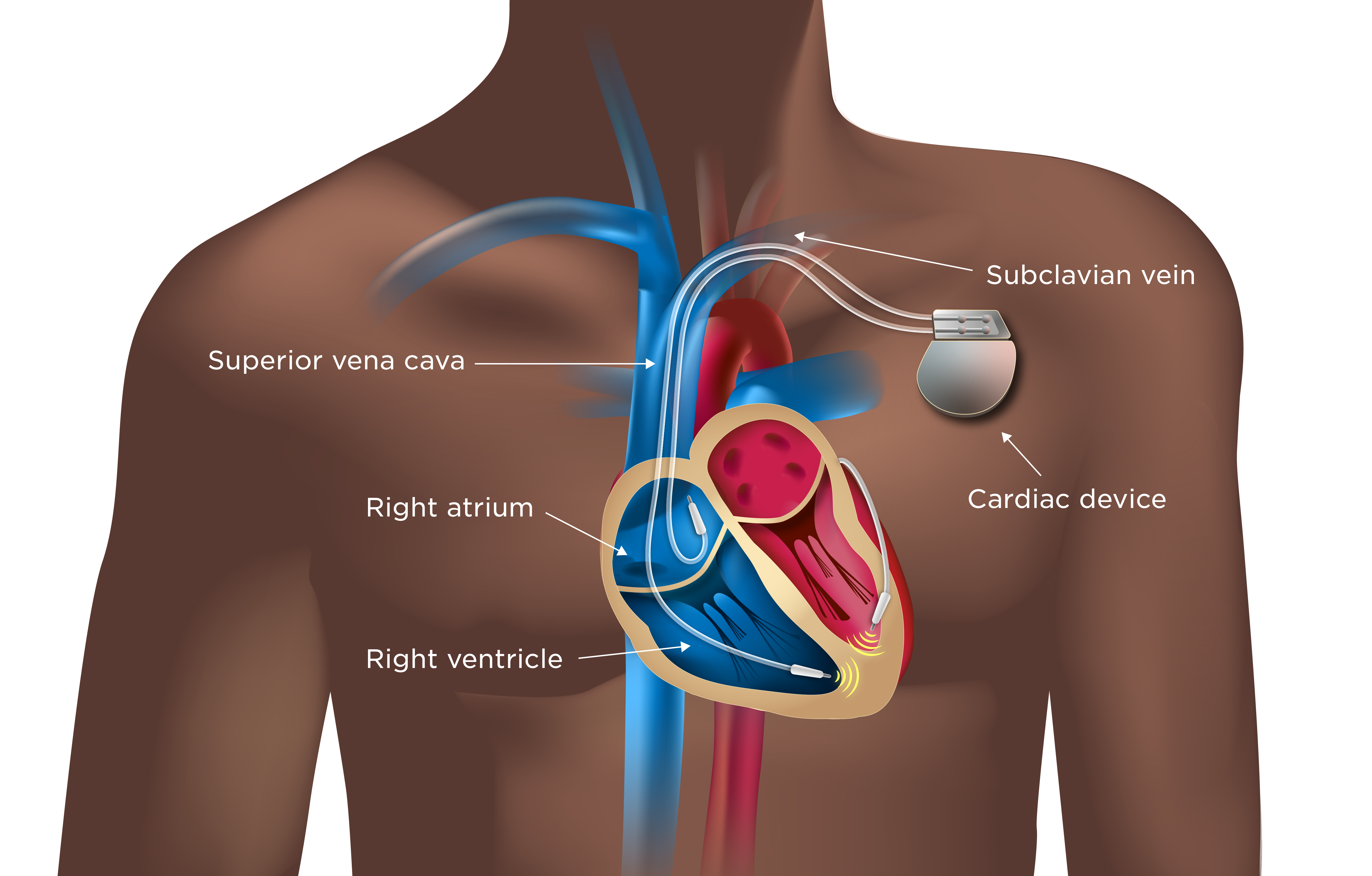
The cath lab has been the steepest part of the learning curve so far. I am working towards competency in several procedures at once: echocardiography, permanent pacemaker implantation, diagnostic coronary angiography, and loop recorder implantation. I can now place loop recorders independently, which feels like a solid early milestone.
Pacemaker implantation brought an unexpected challenge. The procedure involves an incision and pocket closure, and I had not sutured anything since an ED job in F2, roughly four years ago. I went back to basics and got a suturing kit to practise with at home. It made a genuine difference. The first week closing the pocket in the lab, it was effortful; now it feels closer to muscle memory.
The same is starting to happen with the gown and the general theatre environment. Early on, even putting on a surgical gown felt unfamiliar. Now it is automatic. I expect that pattern will repeat as I do more procedures.
In terms of where I am technically: I can get radial access for coronary angiography independently, infiltrate the pacemaker pocket for local anaesthesia, and obtain axillary access under fluoroscopy guidance. Cephalic vein cutdown access is a work in progress. I have successfully positioned an RV lead through the tricuspid valve into the apex under supervision, and I can connect the lead pins to the generator. These are the building blocks, and the pieces are starting to connect.
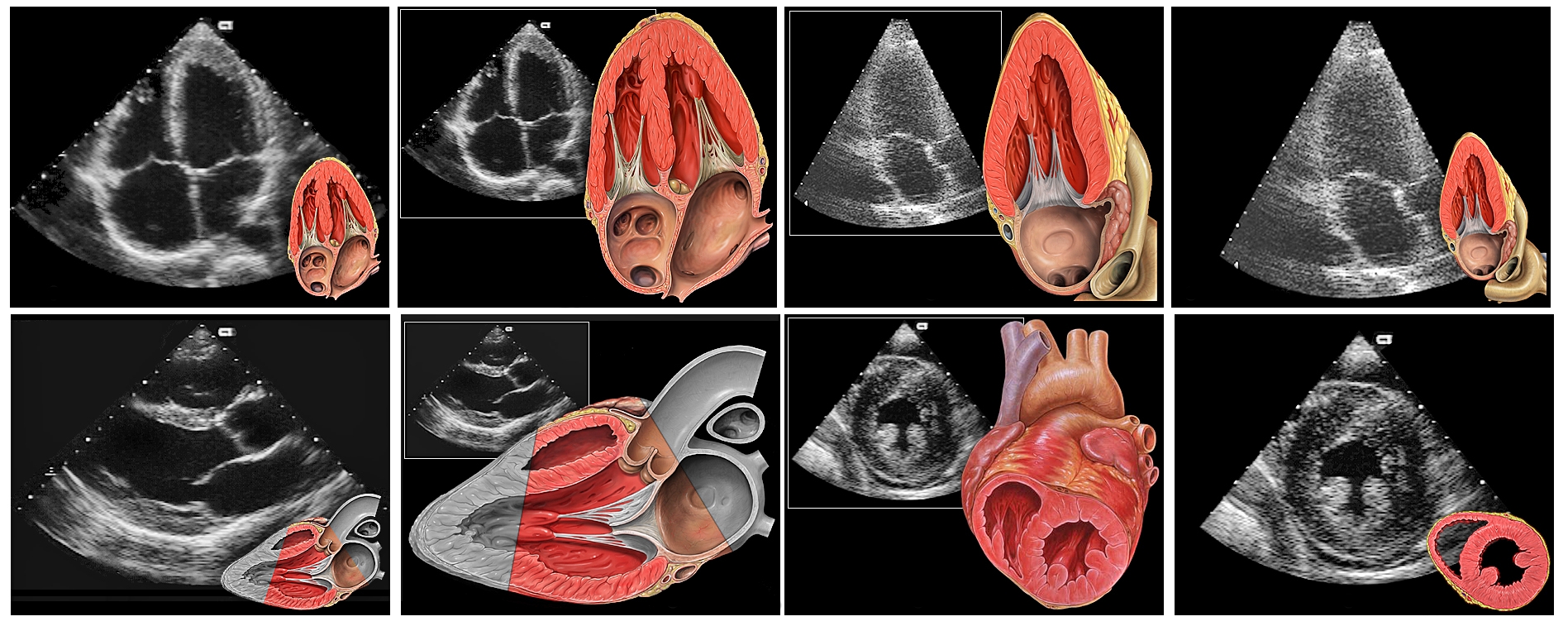
Echo: a work in progress
Echo is coming along, though more slowly. I have a reasonable grasp of the acquisition process and can obtain most standard views, but the subcostal window is still giving me trouble. I am told this is common early on, and I expect it will come with time and repetition. BSE Level 2 accreditation is a longer-term target, and I am treating echo as something to build steadily rather than rush.
Beyond the procedures
One overnight shift stood out in a different way. A patient came in with a large pneumothorax causing significant haemodynamic compromise and needed an urgent chest drain. I completed it safely, without senior backup in the room. She was very grateful afterwards, and it was a good reminder of why these acute skills matter, even in a subspecialty training post.
I have also found that I enjoy the teaching side of the job more than I expected. I have been making a point of supporting the junior doctors on the ward and making sure they have a solid grounding in basic cardiology, not just to help them manage patients, but because I think it makes for better physicians. It does not feel like an extra burden. If anything, it is one of the more satisfying parts of the week.
At the departmental governance meeting in my first month, I presented the mortality review to the consultant body and got good feedback. It was a useful early introduction to how the department thinks about quality and clinical outcomes.
Two months in
Two months into ST4, I think I am having a good time in training. The procedures are coming together, the structure of the week suits me, and there are enough genuinely interesting cases to keep things engaging.
There will be harder stretches ahead. The oncalls are not going to get easier on their own, and there will be procedures that take longer to click than expected. I am aware of that. For now, though, the direction of travel feels right.
Thanks for reading.